When Acute Anterior STEMI Does Not Meet Guidelines
EMS was called to evaluate a male patient in his 60s with a chief complaint of chest pain.
He is found at his residence lying on the couch.
- Onset: Gradual while walking
- Provoke: Initially the pain felt better with rest
- Quality: Described as a dull ache
- Radiate: The pain radiates to the back
- Severity: 7/10
- Time: 3 hours
He states that he feels nauseated and vomited x2 prior to EMS arrival.
Past medical history: Epilepsy, Bladder cancer
Medications: Gabapentin (Neurontin)
No known drug allergies.
Vital signs are assessed.
- RR: 24
- HR: 104
- NIBP: 145/95
- Temp: 98.5 F / 36.9 C
- SpO2: 99% on room air
Breath sounds are clear bilaterally.
There is no jugular venous distension or pitting edema.
The cardiac monitor is attached.

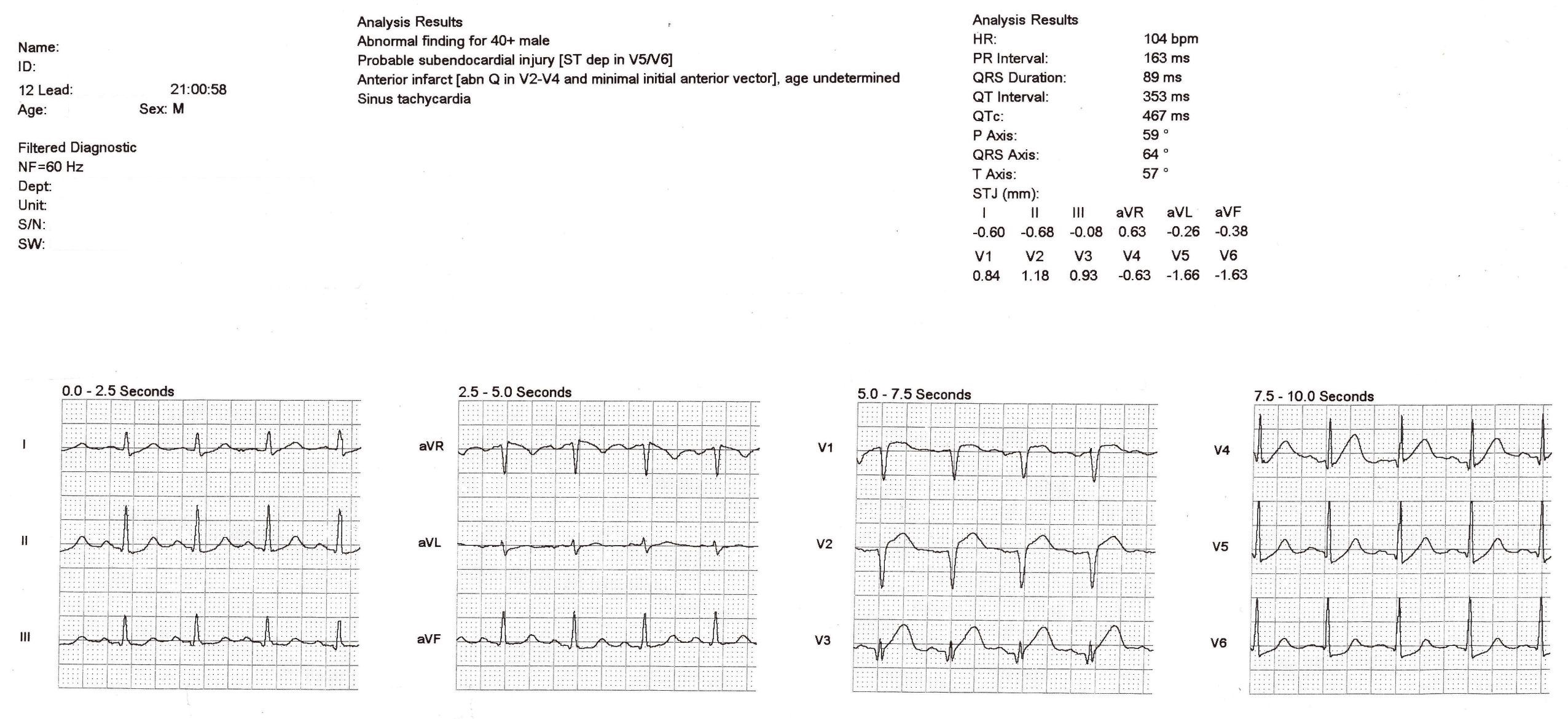
A 12-lead ECG is obtained.
The ECG is determined to be non-diagnostic by the treating paramedic.
The patient is loaded for transport.
The patient again complains of nausea. The treating paramedic withholds aspirin. The patient refuses an IV. Nitroglycerin is withheld. He is transported to the Emergency Department where care is transferred to a nurse.
At the hospital a 12-lead ECG is recorded within 10 minutes and read by the attending physician, who activates the “Code STEMI” protocol.
The paramedic, feeling a bit sheepish, asked me to review the case. Is this a STEMI? The answer is yes! But it does not meet guidelines. So technically it is a STEMI equivalent.

The STEMI guidelines require 2 mm of ST-segment elevation in leads V2 and V3 for men (1.5 mm for women). In this example there is barely 2 mm of ST-segment elevation in lead V2 and no more than 1 mm of ST-segment elevation in lead V3 (measured at the J-point).
Regardless, these T-waves are hyperacute!
“How can that be so?” you might ask. After all, these T-waves aren’t that big.
But they are big compared to the size of the QRS complex! This is known as the rule of proportionality which states that repolarization is proportional to depolarization!
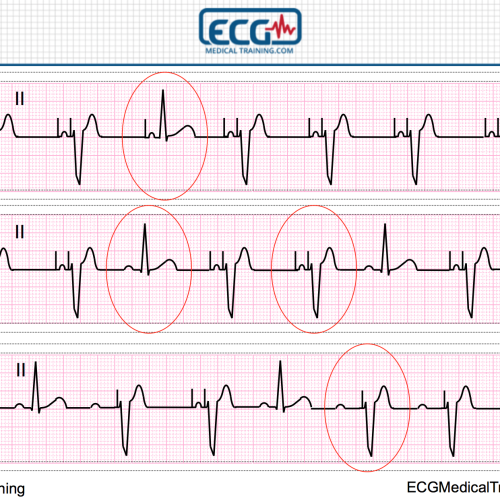
To illustrate this point I’m going to take lead V3 and use PowerPoint to “photo shop” a different QRS complex with deep S-waves onto the exact same ST/T-waves.

Assuming the patient has signs and symptoms of an acute coronary syndrome (you always want clinical correlation), you should consider the T-waves in example A. to be hyperacute and highly concerning for acute STEMI.
In contrast, the T-waves in example B. should be considered perfectly normal relative to the depth of the S-waves. It’s always a judgment call, which is one of the drawbacks to ECG machines that crop the R-waves and S-waves.
Another important feature of this case is the fact that R-wave progression has been obliterated in leads V1-V4. In fact, there are Q-waves in leads V2-V4. In addition, there is ST-segment depression in leads V5 and V6. These findings essentially rule-out early repolarization.
Let’s take a look at the computerized interpretation.

The computer is calling this anterior infarct “age undetermined”. It has often been pointed out that computers are relatively insensitive when it comes to identifying acute STEMI. In reality, it is the guidelines and arbitrary millimeter criteria that are insensitive!
I’m sure some of you are asking, “What about serial 12-lead ECGs?” That’s a great idea! Serial ECGs frequently clinch the diagnosis when the initial 12-lead ECG is non-diagnostic (or, as in this case, does not meet guidelines).
Serial ECGs were reportedly recorded on this call but I have not yet been successful in retrieving them from the database. I will update the case if and when they become available.
Further Reading
Take a look at these blog posts from Dr. Smith’s ECG Blog.
Proportionality and Serial ECGs Make the Diagnosis
Friday’s Post Produced Skeptics…