Ischemia does not localize! What does it mean?
Ischemia Does Not Localize
When it comes to 12-lead ECG interpretation — and STEMI recognition in particular — it’s important to keep in mind that ischemia (as opposed to acute injury) does not localize. This is one of the most important lessons I have learned from Stephen Smith, M.D. from Dr. Smith’s ECG Blog.
We were all taught that ST-segment elevation represents acute injury, whereas ST-segment depression represents subendocardial ischemia.
When ST-segment elevation is present in 2 or more contiguous leads we can “localize” a STEMI.
For example, ST-segment elevation in leads II, III, and aVF indicate inferior STEMI, ST-segment elevation in leads V2, V3, and V4 indicate anterior STEMI, ST-segment elevation in leads V5 and V6 indicate lateral STEMI, and so on.
But what about ST-segment depression that is isolated to specific set of leads?
Take this case I found this in my collection. It’s from about 15 years ago. At that time I did not realize what it showed.
Inferior ST-Segment Depression is Reciprocal to High Lateral STEMI
A 54 year old male presents to EMS with chest pressure. He appears acutely ill. He is pale and diaphoretic. In other words, the pre-test probability of ACS is high.
The following ECG is recorded.

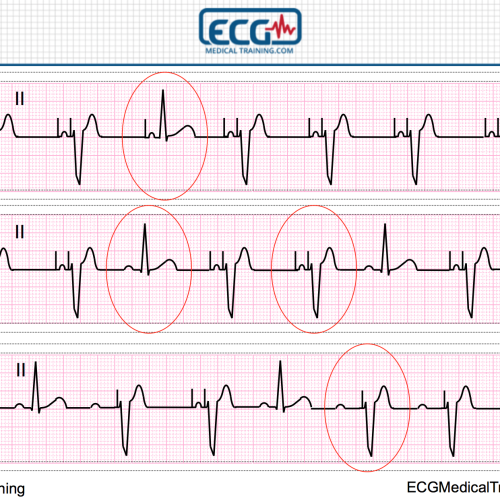
Sinus rhythm with a rate of 86. Downsloping ST-segment depression is noted in the inferior leads. The computerized interpretive statement reads “T-wave abnormality, consider inferior ischemia”.
This must represent inferior ischemia. Right? Not so fast!
Ischemia (unlike acute injury) does not localize on the 12-lead ECG. We know this from cardiac stress testing. It is not axiomatic that the leads showing ST-segment depression correlate with the coronary artery that has stenosis (when it does happen it is probably by chance).
In this case ST-segment depression localized to the inferior leads is more likely to be reciprocal to high lateral STEMI.
“STEMI? Are you nuts! There’s no STEMI on this ECG!”
Keep in mind that leads I and aVL can sometimes be electrocardiographically silent! This is one of those times.
Before you object, let me just say for the record that this ECG does not meet my department’s Code STEMI criteria, and I think most ED physicians would consider me crazy for calling this a STEMI equivalent.
In the actual event the patient received oxygen, aspirin, and nitroglycerin. He was feeling much better by arrival in the Emergency Department.
Here is the 12-lead ECG that was recorded on arrival.

Sinus rhythm with a rate of 91. The ST-segments and T-waves have normalized in the inferior leads. However, reperfusion T-waves are now visible in leads I, aVL, and V2. In addition, the T-waves are much smaller in the precordial leads.
Now there are reperfusion T-waves in leads I, aVL, and V2, strongly suggesting there was an occluded artery. At the time, I did not recognize reperfusion T-waves. I simply thought the oxygen and nitroglycerin “cleaned up” the “inferior ischemia” (especially since the patient felt better).
They’re not all quite this hard. Here’s another ECG that is more typical for electrocardiographically silent high lateral STEMI. The LCX was 100% occluded.

Sinus rhythm with a rate of 71. There is downsloping ST-segment depression in leads II, III, and aVF that is reciprocal to high lateral STEMI.
Anterior ST-Segment Depression is Reciprocal to Posterior STEMI
This was a 70 year old patient with chest pain.

Sinus rhythm with a rate of 67. The R/S ratio in lead V2 is greater than 1. ST-segment depression is noted in leads V1, V2, V3, and V4.
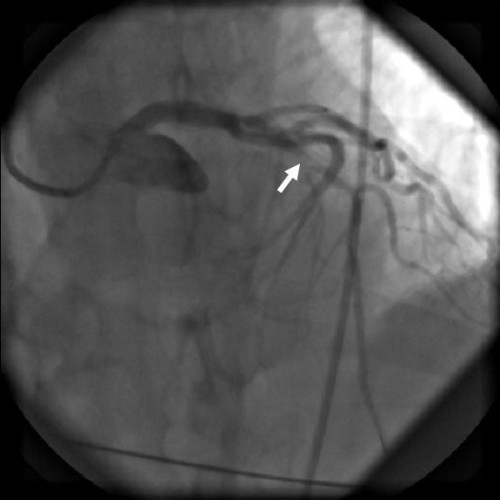
Even though the computerized interpretation is giving the ***ACUTE MI SUSPECTED*** message, the ED physician interpreted this as “anterior ischemia” and the patient was admitted to the ICU. The first Troponin was negative but the second and third were positive. The patient was cathed the next day and had an occluded Obtuse Marginal (OM).
ST-segment depression that is maximal in the right precordial leads (V1, V2, V3) over the left precordial leads (V4, V5, V6) is more likely to be acute isolated posterior STEMI than “anterior ischemia” which is a misnomer!
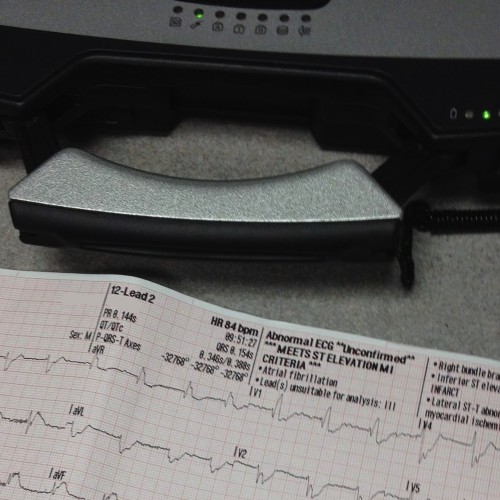
I have found several of these cases over the years during routine QA/QI of cardiac calls. Here’s an example. The data quality is poor but I knew right away I was looking at acute isolated posterior STEMI.

Atrial fibrillation with a rate of 88. There is ST-segment depression in leads V1, V2, V3, and V4.
This was missed by the paramedic, the ED physician, and the cardiologist. The patient was cathed the next day, had a 100% occlusion of the LCX. It was called “Non-ST-Elevation Myocardial Infarction.” As a side note, I am not aware of a hospital that goes out of its way to admit that they missed a STEMI.
Subendocardial Ischemia Should Have Widespread ST-Segment Depression
Subendocardial ischemia on the 12-lead ECG tends to be global. Specifically, there should be ST-segment elevation in lead aVR with widespread ST-segment depression.
Consider this example from anaphylaxis presenting as cardiac ischemia.
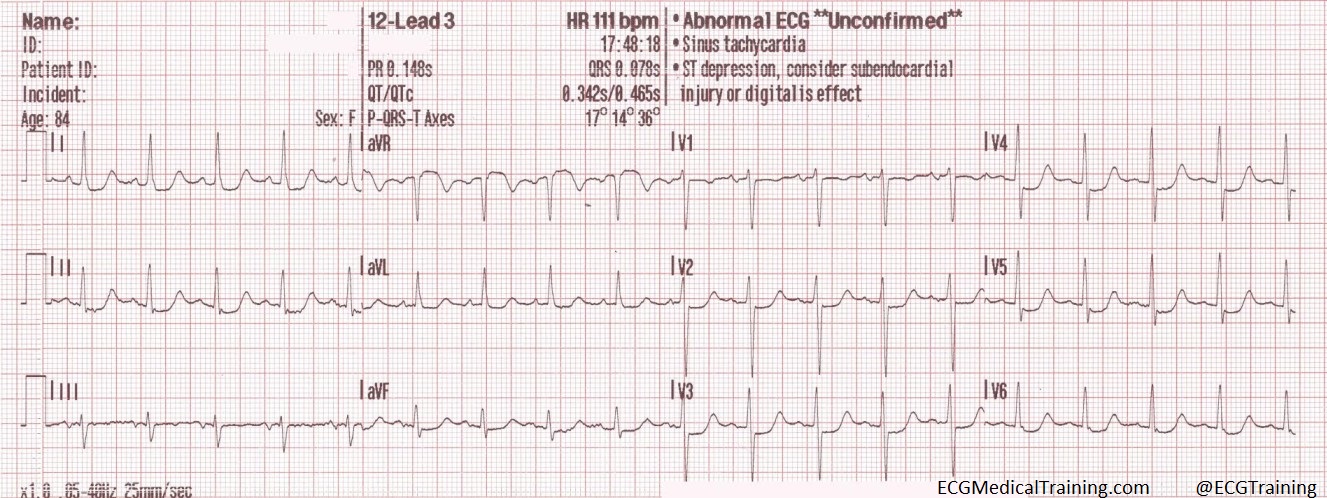
Sinus tachycardia with a rate of 111. ST-segment elevation in lead aVR with widespread ST-segment depression consistent with subendocardial ischemia.
It’s a good idea to eliminate terms like “inferior ischemia” and “anterior ischemia” from your vocabulary! Always think “reciprocal changes” first and “ischemia” second!
Content Reviewer
Stephen Smith, M.D. (@SmithECGBlog)
Further Reading
ST depression limited to inferior leads is reciprocal to high lateral wall and represents STEMI
“Inferior” ST depression: what is the diagnosis?
Isolated posterior STEMI: not rare but often ignored!
Five Primary Patterns of Ischemic ST-Depression Without ST-Elevation. Some Are STEMI Equivalents